The COVID-19 pandemic has had a huge impact on global health and health
systems. It has challenged local, regional, national, and global
capacities to prepare and respond1. The implications significantly altered
aspects of daily life and access to health care, including routine
health services2.
Health systems across the world needed to quickly adapt to the
pandemic3. Due to concerns
about hospital capacity and limited intensive care resources, efforts
were focused primarily on protecting access to critical care services.
Preventive services were reduced, and many preventive and non-urgent
visits were delayed by months or changed to virtual platforms to limit
the need for personal protective equipment use and to limit patients'
and clinical staff's exposure risks. Many people delayed or avoided
seeking routine and even urgent health care services, including nearly
60% of young adults aged 18-24 as shown in one large survey4. This has been shown in
literature, demonstrating decreased outpatient visits provided in 2020,
especially during the period of March- May 20205. As it became evident that the pandemic
would last longer than a few weeks or months, it was clear that primary
health care, including sexual health services, could not be indefinitely
delayed without risking harm.
Millions of new sexually transmitted infections (STIs) are reported every
year in the United States; in 2019 there were 1,808,703 cases of
chlamydia and 616,392 cases of gonorrhea, which were all time high
values. More than half of these infections were among teens and young
adults ages 15-246. Sexually
transmitted infection rates are high in college settings, which
traditionally serve the young adult population. A study examining
chlamydia positivity at college health centers found that college
students were not any less likely than their peers to experience high
rates of chlamydia diagnosis, with rates comparable to those seen in
family planning programs and prenatal clinics7. The long-term consequences of chlamydia
and gonorrhea are frequently underrecognized and include a higher risk
of human immunodeficiency virus (HIV) infection pelvic inflammatory
disease (PID), infertility, and ectopic pregnancy. Screening for
chlamydia has demonstrated reduced rates of PID among women8. Lockdown mandates to
socially distance and self-quarantine were implemented to limit the
spread of COVID-19 throughout the world; while these behavior changes
should have similarly limited spread of STIs, it was unknown to what
extent people were following the recommendations as it pertained to
sexual activity9. For some
young people, social distancing and stay-at-home guidelines have likely
reduced partnered sexual activity10,11. In contrast,
other studies found that sexual activity level stayed the same or
increased, including with new partners or sex outside of one's home12.
Early during the pandemic, US clinical data showed a significant decrease
in the rates of STI visits and treatments13. In addition to this, some surveillance
systems, like in Madrid, Spain, showed a decrease in the reported rate
of STIs when compared to historical data14, whereas other settings found that
despite lockdown orders, rates of STI diagnosis were similar or
unchanged15. Given the known
prevalence of infection and potential for serious consequences of
untreated infection, access to high quality sexual health services is a
key focus of our student health center. While the changes to health
center access were dynamic, particularly during the early days of the
pandemic, making STI testing and treatment accessible to students was a
top priority for UHS.
The University of Wisconsin-Madison (UW) is a large public research
university in the Midwest United States with a total fall 2020
enrollment of 45,540, including undergraduate, master's and doctoral
degree programs16. In 2020,
69.5% of enrolled students were undergraduates, 52.2% were female, 12.9%
were international students, and 65% were white17.
University Health Services (UHS) is a college health clinic that includes
mental health and medical services for UW-Madison students. There are
multiple departments within medical services, including Gynecology,
Sexual Health, and Primary Care. As the primary patients served are
young adults, UHS has had a strong focus on sexually transmitted
infection (STI) diagnosis and treatment in all of these departments. In
2017, a group of nurses specialized in sexual health and an
epidemiologist developed a protocol to assess compliance to follow up
STI testing throughout UHS, showing significant differences within
studied groups18.
Early in the pandemic, it became apparent that the clinic needed to find
a balance between the risks of undetected sexually transmitted
infections for individuals as well as the importance of limiting risks
to staff, patients, and the community associated with having traditional
in-person visits during a pandemic. Limited self-testing appointments
offered by nursing protocol and requiring only a lab visit have been
available to students since 2017. These were initially limited to women
due to limitations with the electronic health record and workflows to be
sure to support the needs of extragenital site testing; extragenital
testing is a routine recommendation for males with male partners (MSM),
in whom only performing genital site testing may miss half or more of
infections19,20,21. This is
particularly worrisome as up to 10% of HIV infections are linked to
chlamydia and gonorrhea infections22. A team at UHS had been looking at
means of expanding this and removing gendered language to be inclusive
but had not yet implemented this before April 2020.
Up until March 13, 2020, clinical access at UHS was normal. After that,
web-booking, the primary means by which patients schedule appointments,
was paused in order to utilize telephone visits as a means of triage by
a nurse or advanced practice provider. While the CDC offered guidance
for STI management with limited clinical interactions in their April
6th, 2020 Dear Colleague Letter23, it was quickly noted by clinicians
that there was an urgency to establish a safe means of testing our
patients; this became a priority for the clinic. Testing for STIs was
deemed appropriate for in-person care again by late March, particularly
for individuals deemed to have higher risk and those with symptoms, but
this process still required a telephone assessment by a nurse or
advanced practice provider first. This was time-consuming and an
additional step to accessing cares. The informatics team, interim deputy
medical director, and sexual health clinicians teamed up to expand
web-booking of STI testing for chlamydia and gonorrhea through a brief
lab visit in order to increase self-test access to patients of any
gender. This was released on April 10, 2020. This was complemented by
ongoing phone triage for people who were experiencing symptoms or were
recommended to complete extragenital screening or blood testing for HIV
and syphilis.
Life on campus was dramatically different during this time period.
Students were advised to move out of dorms during spring break and
classes were moved to virtual only upon return from spring break,
effective March 23, 2020. Classes remained online only through summer
with a mix of online and in-person classes during the majority of fall
semester. Classes returned to online only for the final weeks of fall
semester 2020.
According to unpublished internal campus data, it is estimated that
between 16,457 and 19,751 students remained on campus or the surrounding
areas and were potential users of UHS services during this time.
Historically, over 45,000 students are enrolled per year at UW-Madison
and eligible to utilize UHS. Per state guidelines, as well as for
internal quality improvement initiatives, positive tests for chlamydia
and gonorrhea are routinely tracked. Given all of the changes to
lifestyle and clinical access, we wished to compare the rates of
infection for 2020 following declaration of the global pandemic in March
to preceding years.
The goal of the present study is to assess the impact of the pandemic on
STI testing in a college health setting. To do this we assessed:
- Number of STI tests done during pandemic months
in 2020 compared to historical data and
- Positive rates for STI during pandemic months,
and compared them with historical data and
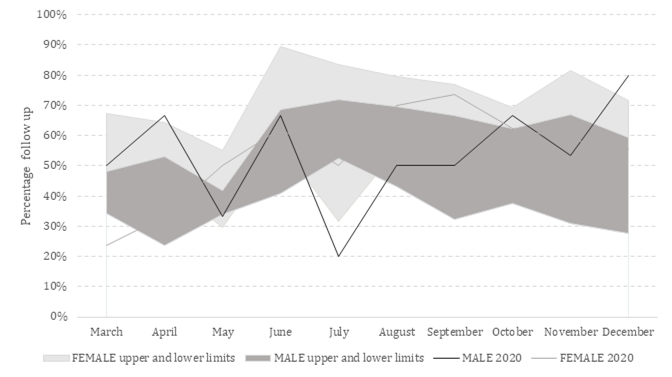
- Percentage of compliance to STI follow up during
pandemic months and compared them with historical data.