Lymphedema is the most serious complication of breast cancer, affecting one in five patients.
The clinical manifestations include swelling of the breast, trunk, and upper limb in the
affected side as well as the impairment and deterioration of limb function, potentially leading
to fibrosis. Psychological sequelae include stressful memories related to the disease,
depression, and anxiety10. We found that the
incidence of lymphedema was four times higher in patients treated by LA (19.9%) than in those
who underwent SLNB only (5.6%)11. Some preventive
measures include skin care and compression in the affected limb dressing; nonetheless, these
measures do not significantly reduce the risk of limphedema development10. These comorbidities have discouraged the use of LA in patients
with negative SLNB, ITCs, or micrometastases as well as in those with positive SLNB treated by
CS according to the ACOSOG Z0011 study criteria. LA in mastectomized patients with
micrometastatic SLNs is common despite evidence from the AMAROS trial showing axillary
recurrence and overall survival being similar between LA and ART. However, the 5-year incidence
of lymphedema is comparatively lower with ART.
Several factors may affect treatment choice, the first being the physician-patient relationship.
Paternalism is developed by physicians who choose the medical procedure that will be performed
because they believe they have the necessary expertise and know what is best for the patient
according to the principle of beneficence. However, the principle of non-maleficence-primum
non nocere-may be unintentionally disregarded, and the choice of LA versus RTA in the
patients of this study is a good example. In the case of axillary treatment for mastectomized
patients, the usual and established procedure before the publication of the AMAROS trial was LA
in cases of axillary SLN involvement in patients with cN0 breast cancer and positive SLNB and
patients with cN1. In many cases, the choice of the most aggressive treatment involves the use
of defensive medicine. Therefore, by choosing LA, the physician ensures that the disease will be
cured, even if it involves overtreatment. This situation involves a bioethical dilemma because
physicians choose to safeguard their reputation without considering the consequences of the most
aggressive treatment on the patient.
In addition, there is a conflict regarding the principle of autonomy. The patient is clarified
via informed consent about the impending procedure. However, the physician does not always offer
the possibility of RTA versus LA to patients who meet the AMAROS trial criteria considering that
the most aggressive treatment is the most appropriate.
Our study evaluated the consequences of using the AMAROS trial criteria in patients undergoing
mastectomy between June 2011 and December 2014. If we had recruited patients after that date
(when lymphadenectomy began to be avoided due to the application of these studies), we would not
have had lymphadenectomy specimens with which to compare the results and show that they could be
unnecessary. These dates were chosen because, based on these principles, the ACOSOG Z0011 trial
criteria were adopted in our center, and LA was not performed in patients with fewer than two
positive SLNs provided that the trial criteria were fulfilled. If the patients had been
recruited at a later date, we would not have had a histopathological result because these nodes
would not have been resected.
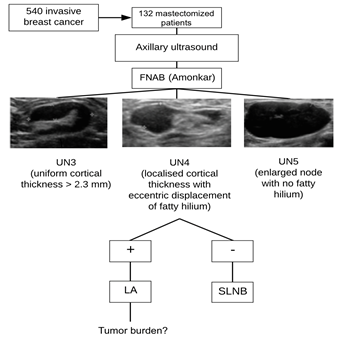
In our center, mastectomy was indicated for 132 of the 405 patients diagnosed with breast cancer
(32.5%), and LA was performed in 58 (44%) patients with metastatic SLNs. 43 (74.1%) of them,
were diagnosed by FNAB, while 15 (25.9%) were diagnosed by SLNB after negative FNAB. Among the
patients who underwent LA, 28 presented a high tumor burden; of them, 26 (92.9%) were diagnosed
by FNAB, while two (7.1%) were diagnosed by SLNB. In one of the patients diagnosed by SLNB,
three lymph nodes were positive in the postoperative histopathological analysis (two nodes plus
one SLN), while six lymph nodes were positive in the other patient (five nodes plus one SLN). Of
the 30 low tumor burden patients treated by LA, 17 (56.7%) were diagnosed by FNAB and 13 (43.3%)
were diagnosed by SLNB. The AMAROS criteria were not applied to this general population.
Nonetheless, if these criteria had been adopted, the 13 LA procedures could have been avoided in
low tumor burden patients diagnosed by SLNB.
Therefore, the sensitivity of FNAB for detecting positive lymph nodes in the population of
mastectomized patients in our series was 93%, while the specificity was 84%. With respect to the
external validity variables, the probability of a high tumor burden in patients with positive
FNAB was 60% (PPV), whereas the probability of a high tumor burden in patients with negative
FNAB was 79% (NPV) (Table 3).
Several studies have shown the ability of ultrasound to diagnose axillary involvement compared
to SLNB. They evaluated tumor characteristics and survival in patients with axillary involvement
diagnosed by FNAB or SLNB12. The patients diagnosed
by FNAB were older and presented palpable masses, larger tumors, higher tumor grade,
lymphovascular invasion, negative hormone receptors, positive HER2, and a higher proportion of
mastectomies compared to the group diagnosed by SLNB. They concluded that patients diagnosed by
FNAB had fewer favorable characteristics and a worse prognosis12. Similar conclusions were made by Boone13, who assessed the tumor burden and disease stage using FNAB or
SLNB and demonstrated that these parameters were worse in patients diagnosed by FNAB. The
results of these two studies are consistent with those of our study, in which the diagnosis of
positive SLNs by FNAB and SLNB in patients with a high tumor burden was 92.9% and 7.1%,
respectively.
With regard to the ultrasound criteria used to identify clinical signs and described by
Amonkar6 (FNAB before the diagnoses of nodes UN3, UN4,
and UN5 in the present study), Ying Zhu et al.14 also obtained a cut-off point greater than 3.5 mm in cortical
lymph node thickness for detecting metastatic infiltration with a sensitivity of 75.6% and
specificity of 82.7%, which, when combined with FNAB, represented a sensitivity of 64.2% and
specificity of 94.5% for detecting metastatic SLNs.
These results were obtained in the total mastectomized population without use of the AMAROS
criteria but can be extrapolated to the population that meets these criteria. Of the 63 selected
patients, SLNB was performed in 61; 51 and 10 of them had negative and positive SLNB,
respectively. Nine of the positive cases presented a low tumor burden and one presented a high
tumor burden; the latter had three positive lymph nodes in LA (one SLN and two other nodes).
Therefore, if AMAROS criteria had been applied to these patients, nine of the 10 (90%) LA
surgeries performed in patients with a low tumor burden could have been avoided.
Most LA procedures performed in the total mastectomized population13 could have been avoided in patients who met the AMAROS trial
criteria9.
In our study, we did not assess the long-term implications of the choice of LA versus ART
because it was retrospective. However, Moossdorff (2018)15 assessed the impact of the AMAROS trial on axillary management
in mastectomized cT1-T2cN0 patients in 2005-2015 in their center and found that 87% of the
patients underwent LA, of whom 61% were also treated by RT after mastectomy. Therefore, ART
could have been used instead of LA in a considerable number of patients.
A prospective study assessed the possibility of replacing LA with ART in mastectomized cT1-T2cN0
patients16. Nonetheless, SLNB was not performed in
patients who underwent post-mastectomy RT. The study concluded that LA could be replaced with
post-mastectomy RT and ART in most patients with fewer than two positive SLNs16.
The morbidities of different axillary management strategies has been analyzed previously17 by comparing the function and mobility of the arm
18 months after surgery in patients treated with LA or RT. The authors found that morbidity was
higher in the group treated with LA17.
Our study has some limitations. First, nodes with ITCs and micrometastases were considered
negative on SLNB (according to the consensus of St Gallen (2009)9), whereas SLNs with micrometastases were considered positive
using the AMAROS trial criteria. However, if the presented data are re-analyzed in the total
population of patients who underwent mastectomy considering these criteria, of the 89 who
performed SLNBs, 55 would be considered negative and 34 would be considered positive; of them,
32 patients would have a low tumor burden and two would have a high tumor burden. The number of
patients with a high tumor burden did not change in this study, whereas the number of patients
with a low tumor burden increased (32 patients whose SLNs contained micrometastases versus 13
patients whose SLNs did not contain micrometastases). These results support the AMAROS trial
criteria because 32 LA procedures could have been avoided. Nodes with micrometastases were
considered positive in the patients who met the AMAROS trial selection criteria. Of the 61
performed SLNBs, 41 biopsies were negative and 20 were positive; of the positive cases, 19
patients had a low tumor burden and one had a high tumor burden. Considering the positive cases,
those with a low tumor burden would increase from nine to 19; therefore, 19 LA procedures could
have been avoided. There were no significant differences in the number of patients with a high
tumor burden.
Another limitation of the AMAROS trial is the lack of consensus regarding in which type of
cT1-T2cN0 patient postmastectomy RT is more indicated. Although the meta-analysis of the Early
Breast Cancer Trialist Cooperative Group showed that this procedure increased overall
survival15, the American Society of Clinical
Oncology/American Society of Radiation Oncology guidelines indicate that the decision regarding
postmastectomy RT should be made on an individual basis15,16,18.
The AMAROS trial excluded multifocal involvement until 2008. They determined19 the SLN detection rate in patients from the AMAROS trial with
multifocal and unifocal involvement. The rate of detection in the first and second groups was
96% and 98%, respectively, and metastatic SLNs were present in 51% and 28% of the patients in
the first and second groups, respectively. However, the involvement of other lymph nodes was
observed in 40% and 39% of the patients from these two groups, respectively, demonstrating that
SLNB is safe in both patient groups. In our population, 68.2% of patients (both in the total
group and the AMAROS trial group) had unifocal involvement.
Another limitation of the AMAROS and ACOSOG Z0011 trials is that most of the enrolled patients
presented positive estrogen receptors and were aged >50 years (with a better prognosis in
both populations). These results were confirmed in our study, in which the mean age of the
patients was 59.7 years in both groups, and the most prevalent molecular pattern was luminal A
(32% and 57% in the AMAROS and total patients, respectively), followed by luminal B HER
2- (11% and 30% in the AMAROS and total patients, respectively). These results
violate the ethical principle of justice because these patients had an improved prognosis.
However, belonging to a molecular group of higher-risk breast cancer and the presence of
estrogen receptors were not exclusion criteria; these results were confirmed in our series
(Tables 1 and 2). However, others have evaluated20
patients with triple-negative (the most aggressive) breast cancer and found that the 5-year
local recurrence rate was low in this population and the main complication was distant
recurrence.
Another factor that affects prognosis is lymphovascular involvement (involvement of the vessels
and lymphatics adjacent to the tumor; therefore, an indicator of poor prognosis). In our series,
this complication did not occur in 71.4% of the women who met the AMAROS criteria or 60.6% of
the total analyzed population.
Another relevant factor is ART-associated morbidity. The side effects included limited shoulder
motion (which was similar between LA and ART2
according to the AMAROS trial results), cardiac and pulmonary toxicity, and the possibility of
secondary tumors with prolonged usage21. In this
study, proton therapy was proposed as an alternative.
In contrast, the majority (77%) of patients from the AMAROS trial had a single positive SLN,
while 40% had SLNs containing micrometastases or ITCs. The patients who underwent NC were
excluded22, and these findings agree with our study
(Table 2).
These results together with patient characteristics and the strict selection of patients who
followed the AMAROS trial recommendations provide excellent evidence that LA should be avoided.
First, only patients with small tumors (cT1-T2) were evaluated and, among them, those who
underwent NC (usually those with a worse molecular prognosis) and had clinically negative
axillary lymph nodes (cN0) were excluded. Therefore, axillary ultrasound plays a fundamental
role in this patient group because it indicates disease prognosis and ultrasound can detect the
clinical stage N0, indicating the importance of this examination for identifying patients with
non-metastatic and micrometastatic SLNs.
However, despite this evidence, there is no consensus regarding axillary surgical management.
For instance, a group evaluated23 compliance with the
clinical guidelines of the ACOSOG Z0011 trial using a survey of 488 surgeons who treated 5,080
early-stage breast cancers between 2013 and 2015. Their study concluded that there were
considerable variations in compliance with significant overtreatment (49% and 63% of surgeons
would recommend LA in the presence of one and two micrometastatic SLNs, respectively). This
study is a clear example of the adoption of paternalism. Most surgeons prefer overtreating over
performing a lower-morbidity technique such as ART24,25.