Exercise dosing considerations in times of COVID-19 pandemic: A review
Consideraciones sobre la dosificación de ejercicio en tiempos de pandemia de COVID-19: Una revisión
How to cite: Carrizo-Largo J, Azócar-Gallardo JW, Ojeda-Aravena A. Exercise dosing considerations in times of COVID-19 pandemic: A review. Univ Salud. 2022; 24(Suppl 1):308-14. DOI: https://doi.org/10.22267/rus.222403.287.
# Abstract
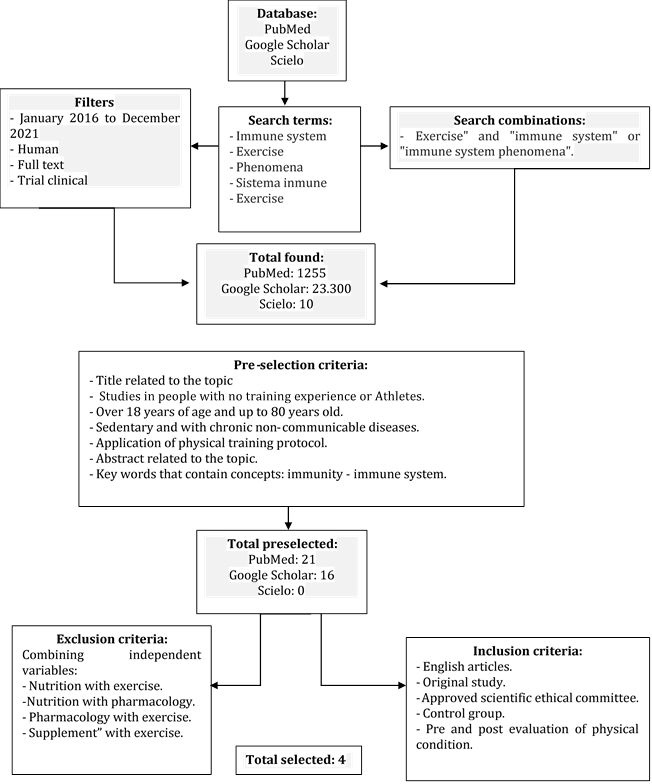
Introduction: During the COVID-19 pandemic, international organizations recommended regular physical exercise to maintain physical and mental health during confinement, however, it is an emerging disease, the evidence is not conclusive regarding the relationship between a physical inactivity and the risk of serious outcomes in patients with COVID-19, therefore, it is essential to identify the contribution of the type of physical exercise modality and the contribution to the immune system. Objective: To demonstrate the immunological response of different physical exercise modality in the population between 18 and 84 years of age, the population identified with the highest number of confirmed cases of COVID-19, in the report n°198 of the World Health Organization. Materials and methods: A review of the literature was carried out between Central Pubmed, Google Scholar and Scielo from January 2016 to December 2021. Results: Of the selected articles, it was possible to identify the main benefits in the immune response with both modalities of physical exercise (aerobic and/or resistance) in the target population. Conclusion: At present, the benefits on the immune response in patients with COVID-19 are completely unknown, which is why it is essential to identify the contribution on the immune response in different modalities of physical exercise in the population between 18-84 years of age.
Keywords: Physical exercise; strength training; resistance training; immune response; immune system; COVID-19.
# Resumen
Introducción: Durante la pandemia de COVID-19, organismos internacionales recomendaron ejercicio físico regular para mantener la salud física y mental durante el confinamiento, sin embargo, al tratarse de una enfermedad emergente, la evidencia no es concluyente en relación a una inactividad física y el riesgo de desenlaces graves en estos pacientes con COVID-19. Es fundamental identificar el aporte del tipo de modalidad de ejercicio físico al sistema inmunológico. Objetivo: Demostrar la respuesta inmunológica de las diferentes modalidades de ejercicio físico en la población de 18 a 84 años, población identificada con mayor número de casos confirmados de COVID-19, en el informe n°198 de la Organización Mundial de la Salud. Materiales y métodos: Revisión de la literatura entre Pubmed Central, Google Scholar y Scielo (enero de 2016 - diciembre de 2021). Resultados: De los artículos seleccionados se identificó los principales beneficios en la respuesta inmune con ambas modalidades de ejercicio físico (aeróbico y/o resistencia) en dicha población. Conclusión: En la actualidad se desconoce por completo los beneficios sobre la respuesta inmune en pacientes con COVID-19, por ello, es fundamental identificar el aporte sobre la respuesta inmune en diferentes modalidades de ejercicio físico en la población entre 18-84 años de edad.
Palabras clave: Ejercicio físico; entrenamiento de fuerza; entrenamiento de resistencia; respuesta inmune; sistema inmune; COVID-19.