Sars-CoV-2 infection rate in employees of a medium and high complexity hospital
Velocidad de la infección con Sars-CoV-2, en funcionarios en un hospital de mediana y alta complejidad
How to cite: Jaramillo-López C, Bergonzoli G, Tinoco-Zapata FJ, Montoya-Restrepo LM. Sars-CoV-2 infection rate in employees of a medium and high complexity hospital. Univ Salud. 2022; 24(Suppl 1):279-86. DOI: https://doi.org/10.22267/rus.222403.283.
# Abstract
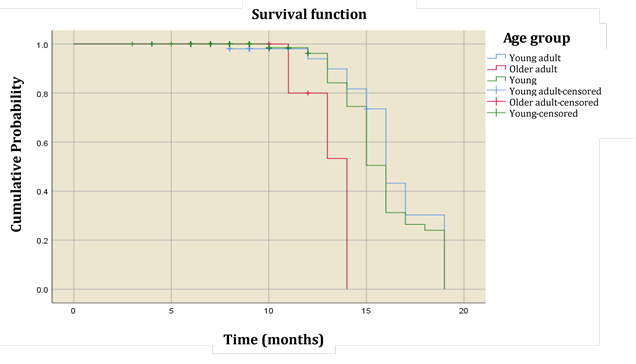
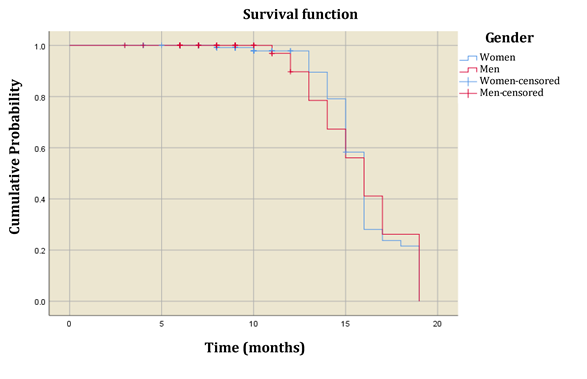
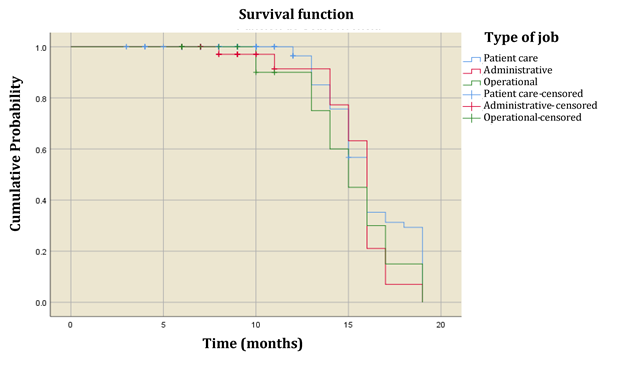
Introduction: The coronavirus disease 2019 (COVID-19) was originally identified in the city of Wuhan, China, in December 2019. Current evidence indicates that the COVID-19-causing virus is transmitted person-to-person through direct contact and droplets. Objective: To estimate Sars-CoV-2 virus infection rate in hospital employees according to their job responsibilities. Materials and methods: Retrospective cohort study to detect Sars-CoV-2 infection in hospital employees, carried out between February 2020 and October 2021. The Kaplan Meier procedure was carried out to estimate the virus infection rate based on variables such as gender, age and job description. Results: There was a difference in infection rate between young and older adult age groups (Log Rank=18.6 gl=1 p≤0.0001). A significant difference was also found between young adult and older adult groups (Log Rank=10.6 gl=1 p=0.0011). Conclusions: The older adult group showed a higher infection rate than that observed in younger age groups. These findings highlight the occupational risk of Sars-CoV-2 infection in health workers, especially in older employees. Therefore, it is necessary to maintain safety measures in order to reduce infection risks.
Keywords: Health care workers; Sars_CoV-2 infection; speed of infection; Kaplan-Meier procedure.
# Resumen
Introducción: La enfermedad por coronavirus 2019 se identificó originalmente en la ciudad de Wuhan, China, en diciembre de 2019. La evidencia actual indica que el virus que causa la COVID-19 se transmite de persona a persona a través del contacto directo y gotitas. Objetivo: Estimar la tasa de infección por el virus Sars-CoV-2 en empleados de hospitales según sus responsabilidades laborales. Materiales y métodos: Estudio de cohorte retrospectivo para detectar infección por Sars-CoV-2 en empleados de hospitales, realizado entre febrero 2020 y octubre 2021. Se realizó el procedimiento de Kaplan Meier para estimar la tasa de infección del virus según género, edad y descripción del trabajo. Resultados: Hubo una diferencia en la tasa de infección entre los grupos de edad de adultos jóvenes y mayores (Log Rank=18,6 gl=1 p≤0,0001). Se encontró una diferencia significativa entre grupos de adultos jóvenes y adultos mayores (Log Rank=10.6 gl=1 p=0.0011). Conclusiones: Los adultos mayores presentaron una tasa de infección superior a la observada en grupos de edades más jóvenes. Se resalta el riesgo ocupacional de infección por Sars-CoV-2 en los trabajadores de la salud, especialmente en los empleados de mayor edad. Es necesario mantener las medidas de seguridad para reducir los riesgos de infección.
Palabras clave: Trabajadores de la salud; infección por Sars_CoV-2; velocidad de infección; Procedimiento de Kaplan-Meier.