Timelines associated with the neonatal jaundice care cycle and assessment of caregiver satisfaction
Tiempos asociados al ciclo de atención de Ictericia neonatal y evaluación de la satisfacción del cuidador
Tempos associados ao ciclo de cuidados da icterícia neonatal e avaliação da satisfação do cuidador
Citation: Noguera LE, Camacho-Cruz J, Vásquez-Hoyos P, Suarez-Cuellar CC, Morales-Lombo AM, Rivera LM, et al. Timelines associated with the neonatal jaundice care cycle and assessment of caregiver satisfaction. Univ Salud [Internet]. 2025; 27(2):e8601. DOI: https://doi.org/10.22267/rus.252702.345.
# Abstract
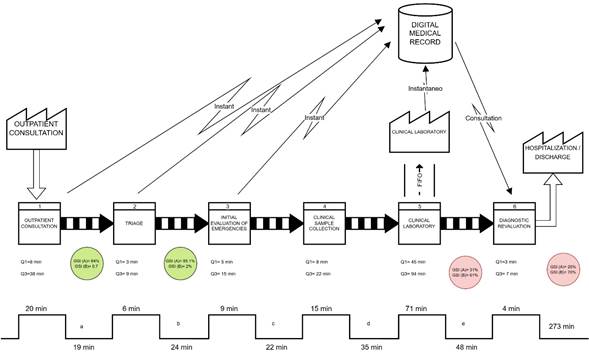
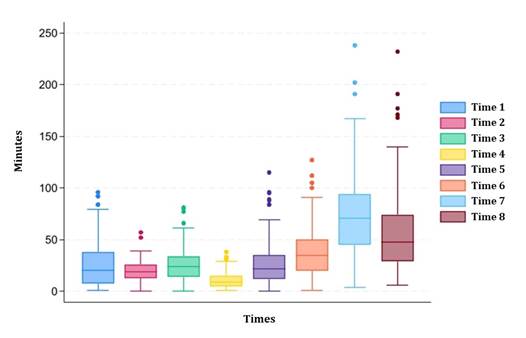
Introduction: Neonatal hyperbilirubinemia is a major health problem, a common cause of morbidity. Worldwide, it affects up to 60% of term newborns. Its diagnosis is by means of serum bilirubin levels, which is associated with certain disadvantages, especially in terms of discomfort related to delayed results. Objective: To evaluate the relationship between caregiver satisfaction and the time associated with the cycle of care for the diagnosis of neonatal jaundice. Materials and methods: Cross-sectional observational study, neonates with clinical evidence of jaundice were included. Demographic data were collected, a satisfaction survey was applied to evaluate the level of caregiver satisfaction, and the times associated with the cycle of care from the moment of admission to the medical procedure were recorded. Results: A patient flow analysis was performed, and it was found that waiting time is significant, especially in obtaining laboratory results. Caregivers' satisfaction with waiting times influences their overall perception of service quality. Conclusions: The potential implementation of new diagnostic instruments could generate added value to the service by speeding up medical decision making.
Keywords: Neonatal jaundice; pediatrics; bilirubin; time. (Source: DeCS, Bireme).
Sustainable development goals: Good health and well-being. (Source: SDG, WHO).
# Resumen
Introducción: La hiperbilirrubinemia neonatal es un problema de salud importante, una causa común de morbilidad. Mundialmente, afecta hasta el 60 % de los recién nacidos a término. Su diagnóstico es clínico y se confirma por medio de la toma de bilirrubinas séricas, que se asocia con ciertas desventajas, especialmente molestias relacionadas con la demora en los resultados. Objetivo: Evaluar la relación entre la satisfacción de los cuidadores y los tiempos asociados al ciclo de atención para el diagnóstico de ictericia neonatal. Materiales y métodos: Estudio observacional transversal, se incluyeron neonatos con evidencia clínica de ictericia. Se recolectaron datos demográficos, se aplicó una encuesta de satisfacción para evaluar el nivel de satisfacción de cuidadores, se registraron los tiempos asociados al ciclo de atención desde el momento de ingreso hasta la toma de la conducta médica. Resultados: Se realizó un análisis del flujo de pacientes y se encontró que el tiempo de espera es significativo, especialmente en la obtención de resultados de laboratorio. La satisfacción de los cuidadores con respecto a los tiempos de espera influye en su percepción general de la calidad del servicio. Conclusión: La implementación potencial de nuevos instrumentos diagnósticos podría generar un valor agregado al servicio, acelerando la toma de decisiones médicas.
Palabras clave: Ictericia neonatal; pediatría; bilirrubina; tiempo. (Fuente: DeCS, Bireme).
Objetivos de desarrollo sostenible: Salud y bienestar. (Fuente: ODS, OMS).
# Resumo
Introdução: A hiperbilirrubinemia neonatal é um grande problema de saúde, uma causa comum de morbidade. Em todo o mundo, afeta até 60% dos recém-nascidos a termo. Seu diagnóstico é feito através da dosagem da bilirrubina sérica, o que traz algumas desvantagens, principalmente o desconforto relacionado à demora na obtenção dos resultados. Objetivo: Avaliar a relação entre a satisfação do cuidador e o tempo associado ao ciclo de cuidados para o diagnóstico de icterícia neonatal. Materiais e métodos: Estudo observacional transversal, foram incluídos neonatos com evidência clínica de icterícia. Dados demográficos foram coletados, uma pesquisa de satisfação foi aplicada para avaliar a satisfação do cuidador e o tempo associado ao ciclo de cuidados foi registrado desde o momento da admissão até o início do tratamento médico. Resultados: Foi realizada uma análise do fluxo de pacientes e constatou-se que o tempo de espera é significativo, principalmente para obtenção de resultados laboratoriais. A satisfação dos cuidadores com os tempos de espera influencia sua percepção geral da qualidade do serviço. Conclusão: A potencial implementação de novos instrumentos diagnósticos poderá gerar valor agregado ao serviço, agilizando a tomada de decisão médica.
Palavras-chave: Icterícia neonatal; pediatria; bilirrubina; tempo. (Fonte: DeCS, Bireme).
Metas de Desenvolvimento Sustentável: Saúde e bem-estar. (Fonte: ODS, OMS).