Helicobacter pylori resistome analysis in Colombia
Análisis del resistoma de Helicobacter pylori en Colombia
Análise do resistoma de Helicobacter pylori na Colômbia

Citation: Guzmán-Bastidas KA, López-Daza SF. Análisis del resistoma de Helicobacter pylori en Colombia. Univ Salud [Internet]. 2026; 28(1):e9569. DOI: 10.22267/rus.262801.352.
# ABSTRACT
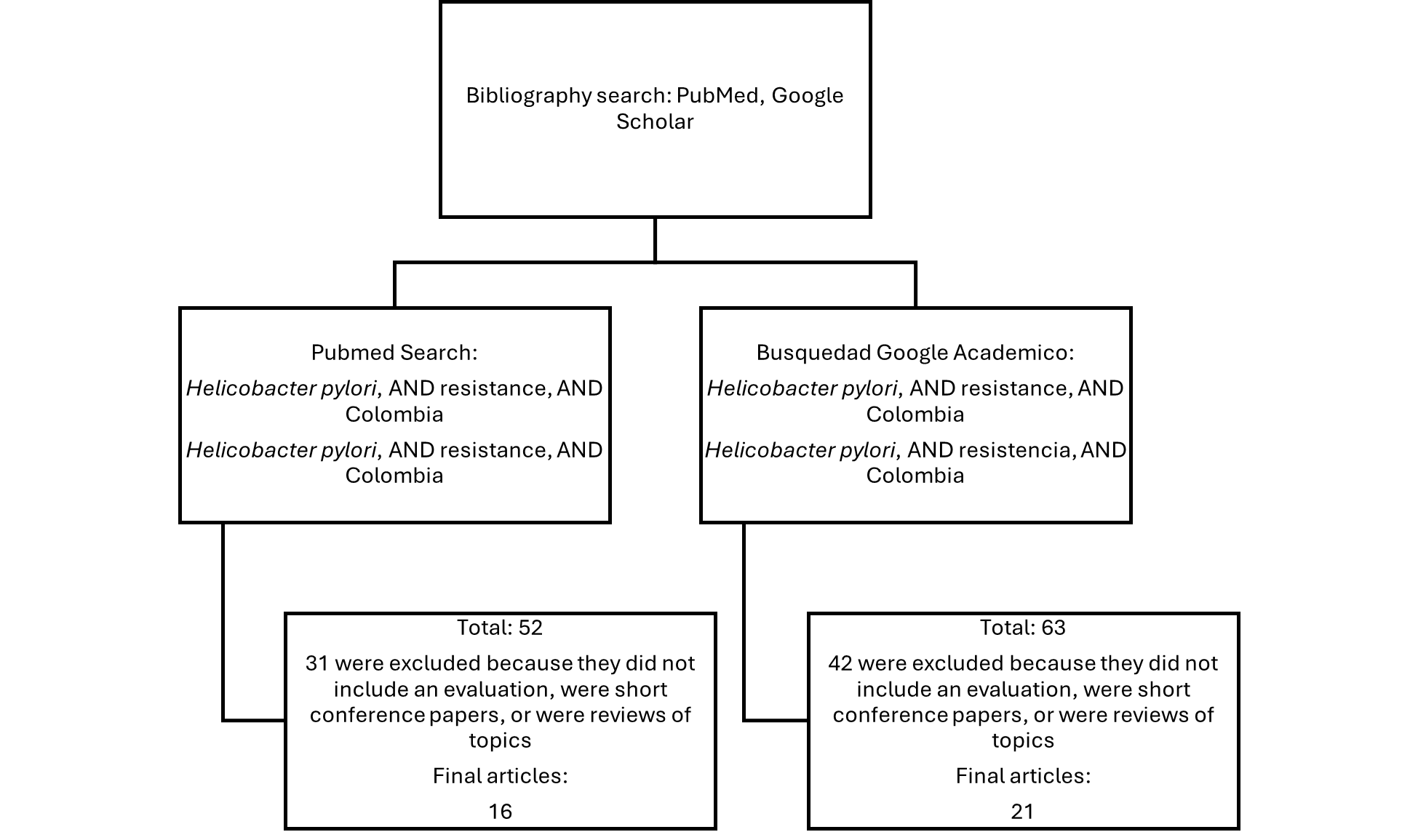
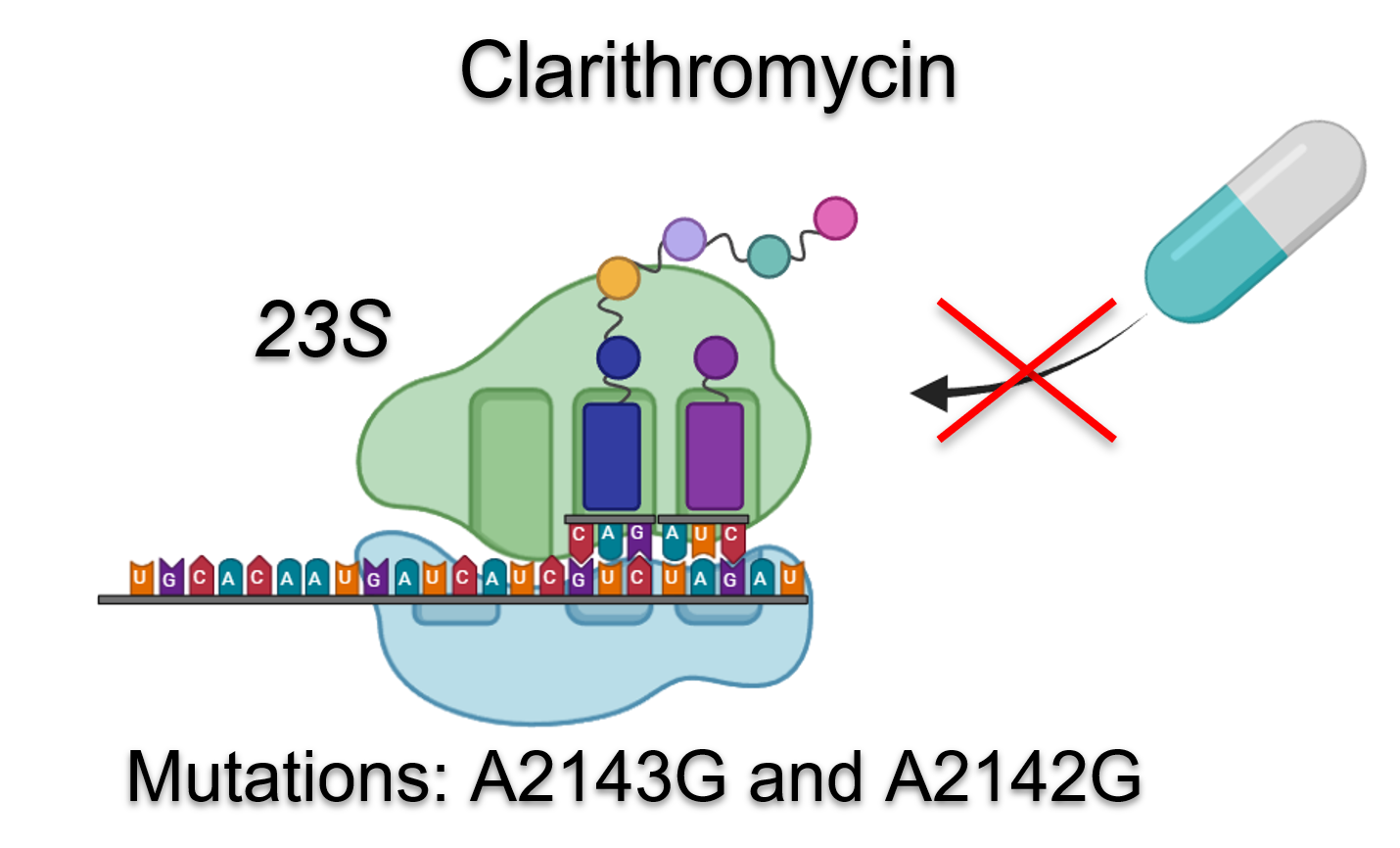
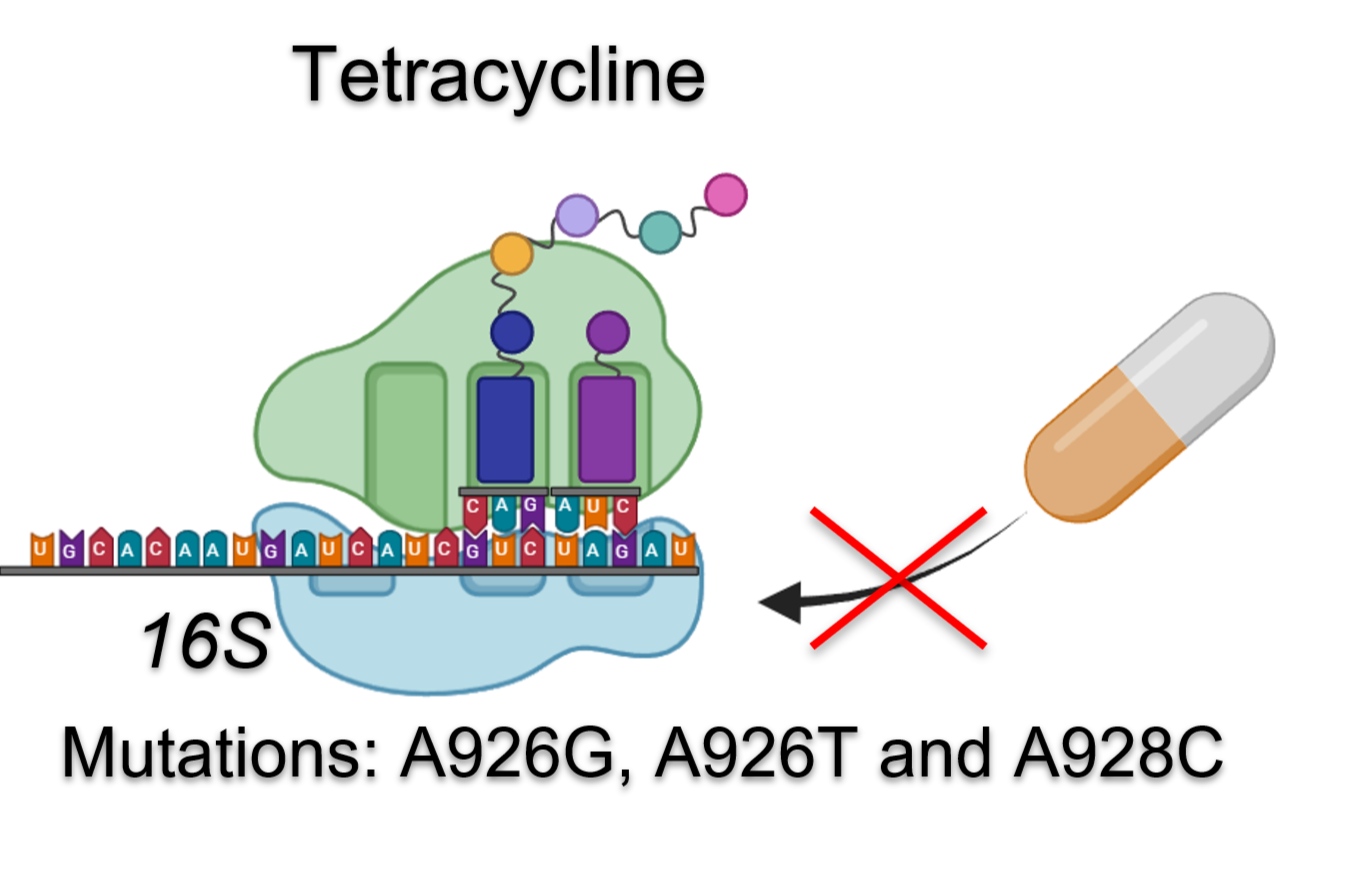
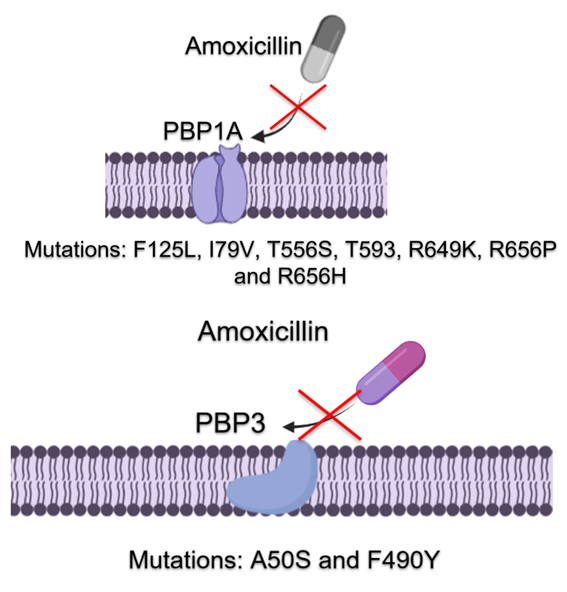
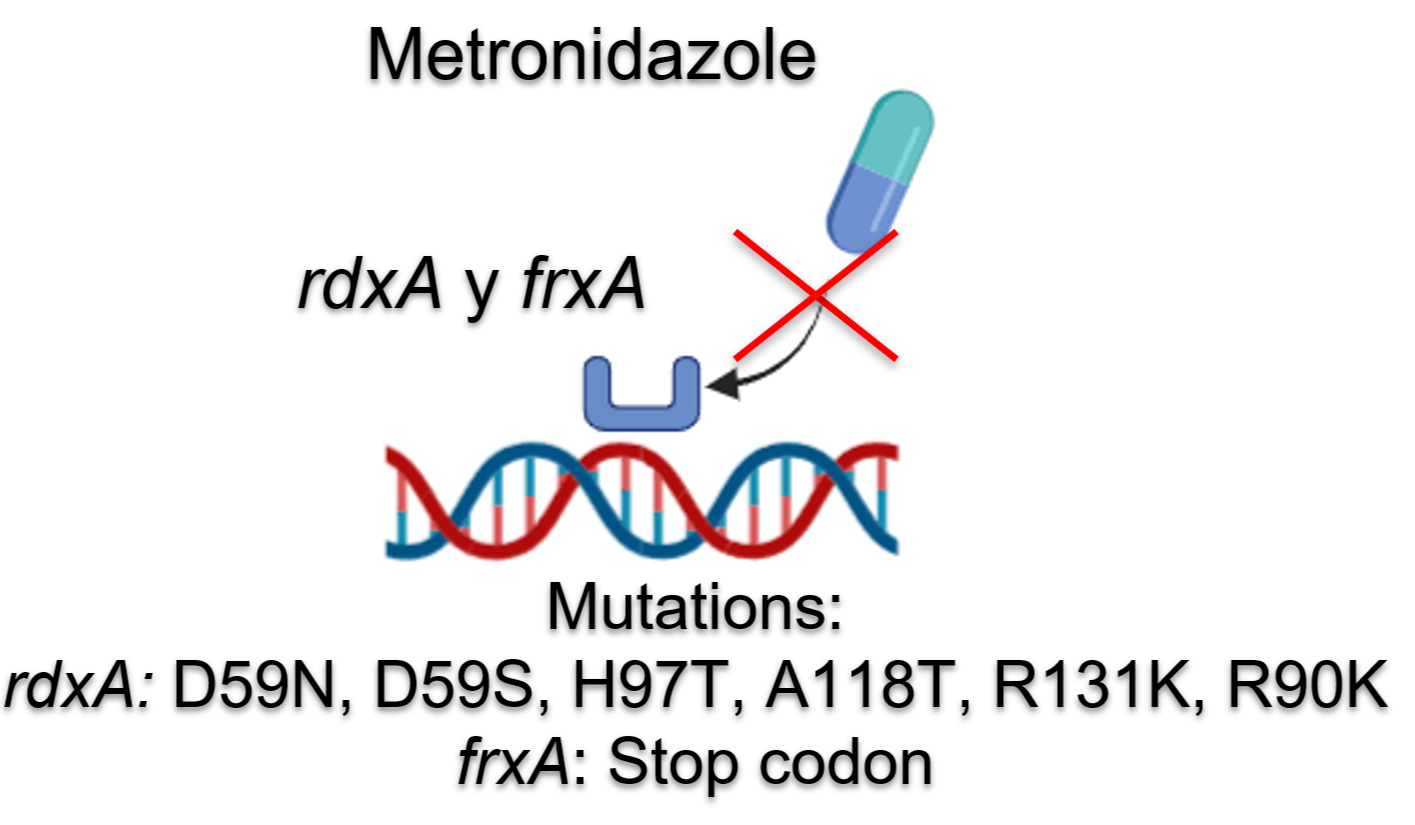
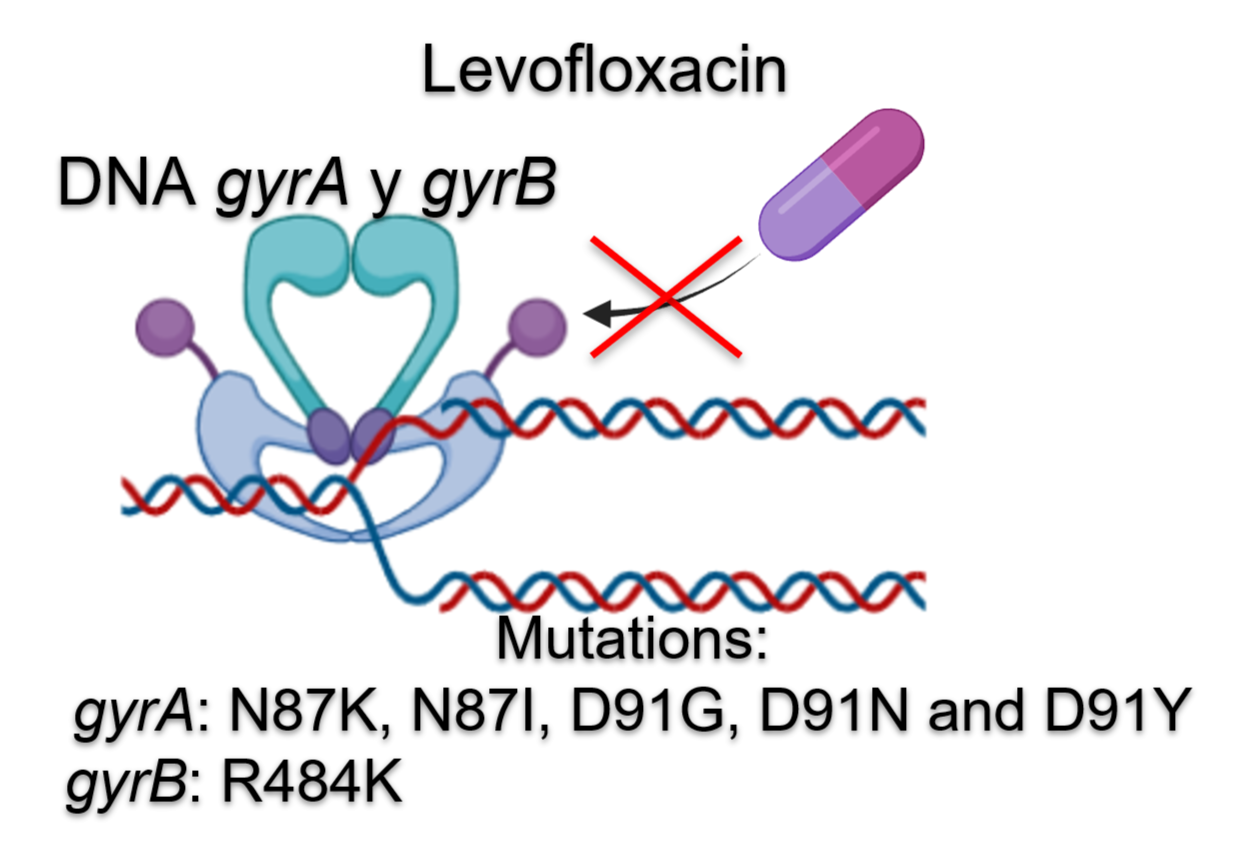
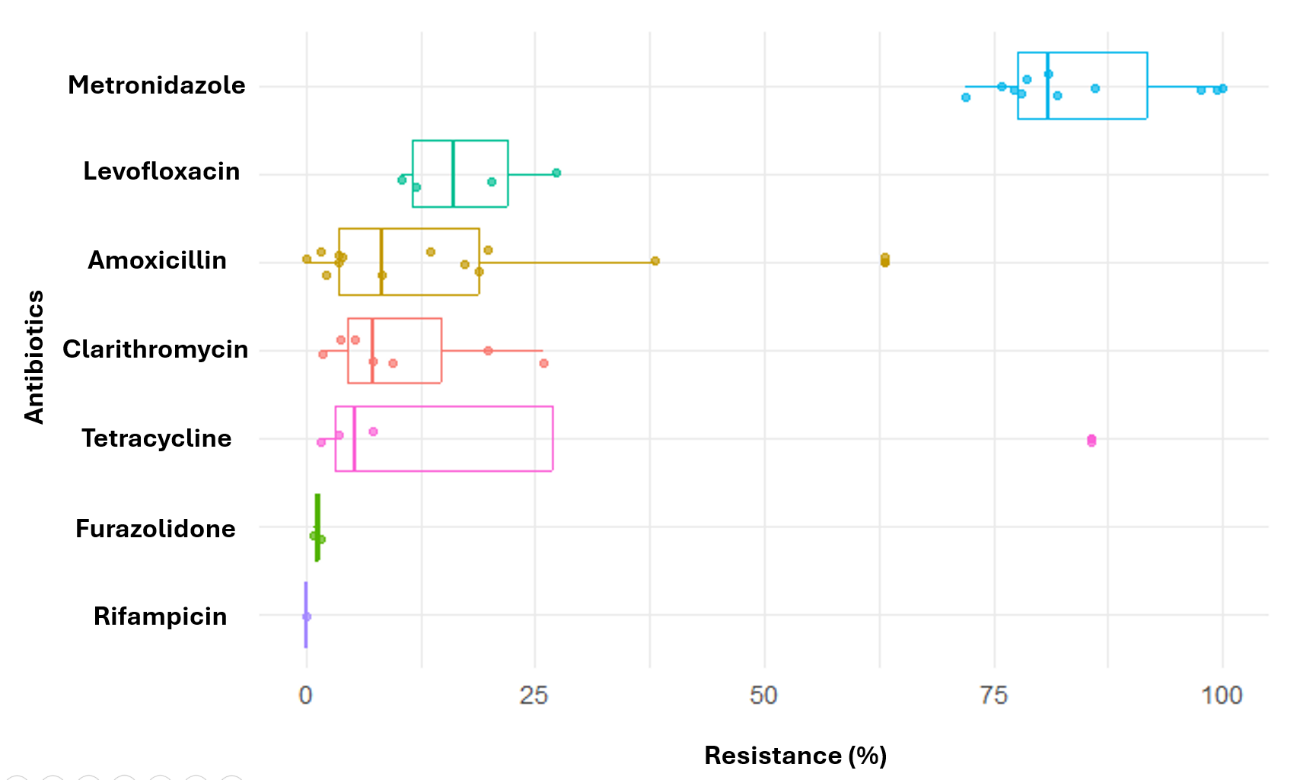
Introduction: Helicobacter pylori is a bacterium closely associated with chronic gastritis and gastric cancer. In Colombia, its high prevalence, along with marked geographical differences in gastric cancer incidence, has prompted studies focused on the antimicrobial resistance of this bacterium. Objective: To characterize the resistome of Helicobacter pylori in Colombia through the analysis of phenotypic and genotypic studies, in order to evaluate resistance pa erns. Materials and Methods: A systematic review was conducted in scientific databases, selecting 21 original studies. Mutations in resistance-associated genes were evaluated, and a descriptive statistical analysis was performed using R software. Results: High resistance to metronidazole was identified, along with variable resistance to clarithromycin and tetracycline, moderate resistance to amoxicillin and levofloxacin, and low resistance to furazolidone and rifampicin. Conclusion: The high resistance to metronidazole excludes it as a reliable first-line option. The variable resistance to clarithromycin and tetracycline requires regional susceptibility testing. Amoxicillin and levofloxacin retain moderate efficacy, while furazolidone and rifampicin stand out as promising alternatives. It is essential to implement phenotypic or genotypic susceptibility testing prior to treatment and to update empirical guidelines based on local resistance surveillance.
Keywords: Antibiotic resistance; Helicobacter pylori; Gastric cancer; Colombia (Source: DeCS, Bireme).
Sustainable development goals: Good health and well-being. (Source: SDG, WHO).
# RESUMEN
Introducción: Helicobacter pylori es una bacteria estrechamente relacionada con la gastritis crónica y el cáncer gástrico. En Colombia, su alta prevalencia, junto con las marcadas diferencias geográficas en la incidencia del cáncer gástrico, han motivado estudios centrados en la resistencia antimicrobiana de esta bacteria. Objetivo: Caracterizar el resistoma de Helicobacter pylori en Colombia a través del análisis de estudios fenotípicos y genotípicos, con el fin de evaluar los patrones de resistencia. Materiales y métodos: Se realizó una revisión de tema en bases de datos científicas, seleccionando 21 estudios originales. Se evaluaron mutaciones en genes asociados a resistencia y se llevó a cabo un análisis estadístico descriptivo utilizando el software R. Resultados: Se identificó una alta resistencia a metronidazol, resistencia variable a claritromicina y tetraciclina, resistencia moderada a amoxicilina y levofloxacina y baja resistencia a furazolidona y rifampicina. Conclusión: La alta resistencia al metronidazol lo descarta como opción fiable de primera línea. La resistencia variable a claritromicina y tetraciclina demanda pruebas de susceptibilidad regionales. La amoxicilina y levofloxacina mantienen eficacia moderada, mientras que furazolidona y rifampicina destacan como alternativas prometedoras. Es fundamental implementar pruebas fenotípicas o genotípicas antes del tratamiento y actualizar guías empíricas basadas en vigilancia local.
Palabras clave: Resistencia a antibióticos; Helicobacter pylori; Cáncer gástrico; Colombia (Fuente: DeCS, Bireme).
Objetivo de desarrollo sostenible: Salud y bienestar. (Fuente: ODS, OMS).
# RESUMO
Introdução: Helicobacter pylori é uma bactéria intimamente associada à gastrite crônica e ao câncer gástrico. Na Colômbia, sua alta prevalência, juntamente com marcantes diferenças geográficas na incidência de câncer gástrico, motivou estudos focados na resistência antimicrobiana dessa bactéria. Objetivo: Caracterizar o resistoma do Helicobacter pylori na Colômbia por meio da análise de estudos fenotípicos e genotípicos, a fim de avaliar os padrões de resistência. Materiais e métodos: Foi realizada uma revisão da literatura em bases de dados científicas, selecionando-se 21 estudos originais. Foram avaliadas mutações em genes associados à resistência e realizada uma análise estatística descritiva utilizando o software R. Resultados: Foram identificadas alta resistência ao metronidazol, resistência variável à claritromicina e tetraciclina, resistência moderada à amoxicilina e levofloxacina e baixa resistência à furazolidona e rifampicina. Conclusão: A alta resistência ao metronidazol o descarta como uma opção confiável de primeira linha. A resistência variável à claritromicina e à tetraciclina exige testes de suscetibilidade regionais. A amoxicilina e a levofloxacina mantêm eficácia moderada, enquanto a furazolidona e a rifampicina se destacam como alternativas promissoras. É essencial implementar testes fenotípicos ou genotípicos antes do tratamento e atualizar as diretrizes empíricas com base na vigilância local.
Palavras-chave: Resistência a antibióticos; Helicobacter pylori; Câncer Gástrico; Colômbia (Fonte: DeCS, Bireme).
Metas de desenvolvimiento sustentavel: Saúde e bem-estar. (Fonte: MDS, OMS).